






- Cactus Conservation Institute Clarification Note about Decriminalize Nature Claims - June 14, 2022
- A Word in Edgewise About the Sustainability of Peyote - May 12, 2020
- Peyote in the United States: Prisoner of War as the War Wanes - November 20, 2017
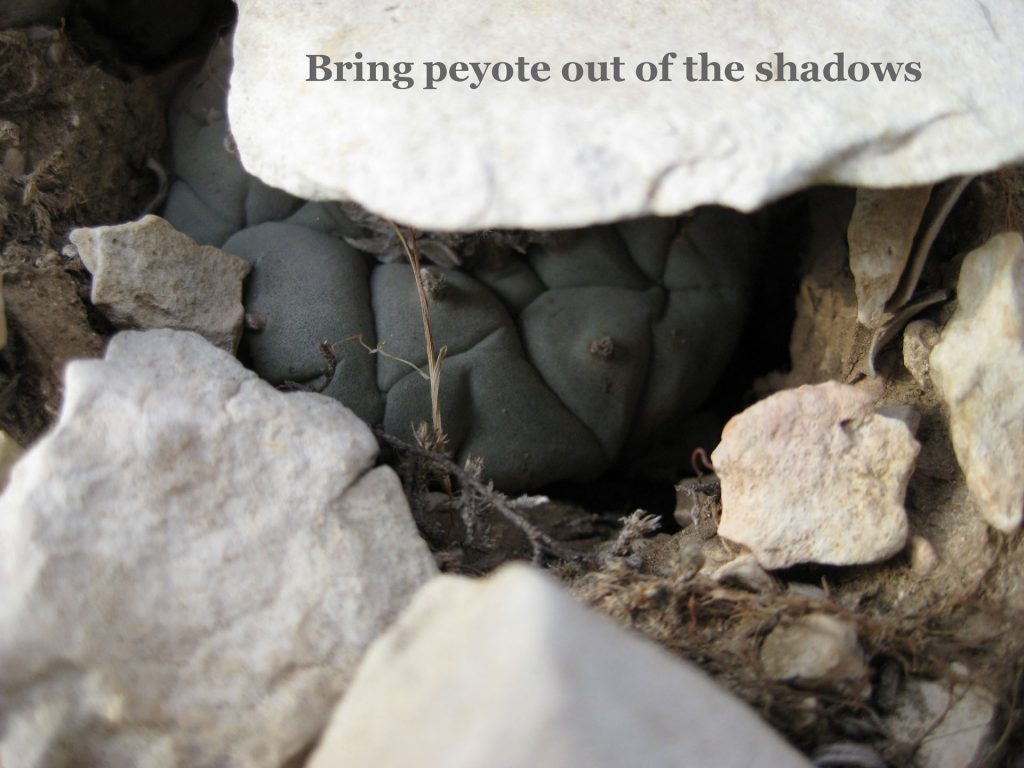
Peyote (Lophophora williamsii) is a small cactus of the Chihuahuan Desert that has a history of human use dating back at least 6,000 year. 1 Currently, its principal uses are medicinal sensu lato, including ceremonial use in meetings of the Native American Church (NAC), an organization which was founded in Oklahoma in 1918 (Stewart, 1987) and has subsequently spread to include congregations throughout the 50 states as well as Canada (Terry, personal observation).
In the USA, the use of peyote by American Indians (or anyone else) was not widely known outside the tribal cultures— although official efforts were made to publicize and demonize it by one Bureau of Indian Affairs agent,2 in much the same spirit as cannabis was later vigorously demonized by a single individual in the federal government in the 1930’s and ’40’s3― until the 1950’s, when Aldous Huxley published The Doors of Perception (1954) and the Beat Generation discovered the psychoactive effects of peyote and its principal alkaloid, mescaline.4 As the Beatniks, who were always a small artistic and literary subculture constituting only a tiny fraction of the U.S. population, gradually faded from the scene, they were replaced in the 1960’s and ’70’s by a new “counterculture” that included the Hippies— essentially, a demographically numerous and highly vocal generation of young people who espoused quite different values from those of the dominant culture with which they reluctantly shared the country. Among those values, clearly articulated in the pop music and literature of the time,5 was an often sophisticated taste for a spectrum of psychoactive drugs which the cognoscenti of the counterculture referred to as “psychedelics” (drugs that expanded the mind)— which, of course, included peyote.

As the 1960’s progressed, several forces came to bear on peyote and its regulation:
(1) Drug use in general increased in the U.S., due in part to the counterculture’s openness to experimentation with drugs for their psychoactive effects, and also due to the exposure to drugs, particularly cannabis and opiates, that occurred on a massive scale among U.S. soldiers in the war in Viet Nam.
(2) In addition to the “baseline” level of peyote harvesting by American Indians for their ceremonial use, in the 1960’s, the wild peyote populations were invaded by non-Indians of the counterculture, seeking peyote for their own use, some of which could be described as ceremonial, spiritual or educational, and some of which was described pejoratively as “recreational.” This increased level of harvesting in the wild peyote populations resulted in the gradual decimation of those populations, which even now remain the only source of peyote for all human uses. The increased harvesting—generally by trespassing—also created animosity between the uninvited harvesters and the ranchers on whose land the peyote grew. Another effect of increased harvesting of peyote from the limited―and shrinking―area of land where peyote grew in commercial quantities, was a subtle one that did not begin to emerge visibly until the 1990’s, and that was the gradual realization among many American Indians that peyote was in short supply. Indeed, by the first decade of the twenty-first century, the sacramental quality of peyote had deteriorated, as the employees of the licensed peyote distributors were harvesting mostly small regrowth buttons that had largely replaced mature peyote plants in the accessible South Texas populations, and some Road Men (spiritual leaders who lead the NAC peyote meetings) were finding it difficult to obtain adequate supplies of peyote for their own NAC members, and therefore they no longer had the luxury of being able to invite non-NAC members into their ceremonies. When this meant, as it often did, that white people were no longer welcome in Indian NAC meetings, the result was the loss of a socioreligious meeting venue where trans-cultural understanding and harmony could be achieved between whites and Indians.
(3) Paranoia about alleged harmful effects of psychedelics, enhanced by ignorance about the pharmacology of psychedelics on the part of the U.S. cultural mainstream, chronically infected the ruling class/generation as the gap between the mainstream culture and the counterculture widened, largely due to differences in perception and experience of the psychedelics per se, and to the increasing volume and stridency of U.S. domestic protest against the Vietnam War, particularly on the part of the younger generation.
(4) The Controlled Substances Act of 1970 (CSA) was the dominant culture’s presumptive solution to “the Drug Problem.” It had a number of flaws, however, and one of them was classifying peyote as a Schedule 1 controlled substance, defined as a substance that has “no accepted medical use and a high potential for abuse.”6 That compound error by the U.S. Congress and the congressional advisors could be attributed to a mistaken lumping together of peyote and LSD as “hallucinogens”, the prejudice and ignorance about peyote on the part of all parties involved in framing the legislation, and the haste with which the CSA was thrown together by the advisors and rubber-stamped by the Congress, which was more interested in “solving the drug problem” with legislation that would appeal to the beliefs of their constituents, than they were in discovering the truth (both pharmacological and cultural) about peyote.

The clearest manifestation of the latter observation is the way Congress dealt with “the Native American problem” in framing the CSA and subsequent peyote legislation. The “inconvenient truth” was that the Native Americans—who were becoming increasingly vocal and politically powerful—had been using peyote legally in the U.S. ever since the NAC was established in Oklahoma in 1918, and some tribes (e.g., the Comanche and the Caddo) could point to their oral histories as evidence that their use of peyote went back several centuries before that. The American Indians made a strong case to the Congress, in the discussions leading up to the American Indian Religious Freedom Act Amendments of 1994 (AIRFAA), that their ceremonial or “religious” use of peyote was protected by the First Amendment of the U.S. Constitution and should not therefore be subject to the prohibition of peyote use that was imposed in the Controlled Substances Act. The Native Americans were victorious in the end, and Congress included in the AIRFAA an exemption for “the nondrug use of peyote in bona fide religious ceremonies of the [NAC].” And yet, peyote (the plant) and mescaline (the predominant alkaloid in the plant) remained in Schedule 1—the same schedule that included LSD and heroin—indicating that peyote was still considered to be a “dangerous drug” under federal law.
Carrying the logic one step further, the classification of peyote as a Schedule 1 drug, plus the AIRFAA language that explicitly provided an exemption allowing the continued use of peyote by American Indians, means that Congress was claiming that peyote is a dangerous drug for white people but is perfectly safe and wholesome for American Indians, irrespective of whether their tribe or group had ever actually used peyote historically or not. What a fascinating pharmacological anomaly! Or was it that Congressional scientists had discovered that American Indians have the miraculous genetic advantage of a unique peyote-detoxification gene that protects them from the ravages of peyote?
Congress had, for reasons unfettered by facts, long viewed peyote as an addictive substance. The clear provisions for those habituated to peyote becoming committed to the federal Narcotics Farms were included in the original legislation creating those facilities.7
That Congressional presupposition of a factually false notion was perfectly compatible with the CSA classification of peyote as Schedule 1 because of its alleged “high potential for abuse.” That claim that peyote is addictive has never been substantiated scientifically. On the contrary, it is universally recognized, both by members of the NAC and by experts in the modern medical community, that peyote is not addictive, as can be evidenced by the fact that peyote ceremonies are never scheduled for several consecutive days; they are normally held at most once a week, and, for many NAC groups, once a month or even less frequently.8 The usual pattern of the peyote ingestion by NAC users is limited to within peyote ceremonies. Such low frequency of self-administration is clearly not compatible with the patterns of use typical of an addictive drug.
Regarding the question of whether any neurotoxicity is caused by the infrequent use of peyote in ceremonies, the data from a study designed to address this question suggest a lack of neurotoxicity in NAC members using peyote ceremonially on a regular basis.9 In a study of hospital records of an urban population of what appear to be non-NAC members who sought medical attention after self-administration of peyote or mescaline, the authors concluded: “Most peyote intoxications appear to be mild in nature and are unlikely to produce life-threatening symptoms.” The most common clinical sign observed was tachycardia (to be expected from the structure of the mescaline molecule and the well-documented activity of structurally related phenethylamines), and the most common clinical symptom noted in the study was “hallucinations.”10 The proposition that the unknowing participants in the latter study were non-NAC members is supported by the fact that, to our knowledge, hallucinations are never reported by NAC participants in peyote ceremonies.
Classification in Schedule 1 also denotes that the drug in question “has no accepted medical use in the United States.” The classification of peyote as Schedule 1 by the U.S. Congress in 1970 raises an important question: Who failed to accept the medical uses (plural!) of peyote over at least the last 500 years (and arguably the last 6,000 years), and why? Even the name of the peyote plant in several tribal languages is the same as the word for medicine. Furthermore, in modern American English, members of the Native American Church consistently use the word “medicine” to refer to peyote. There is a substantial literature on the therapeutic uses of peyote among the American Indian tribes11 (e.g., Schultes 1938, 1940). There are also clear descriptions of bona fide medical uses of peyote in the sixteenth-century Spanish literature.12 At present, there are widespread uses of peyote as topical tinctures, oils (aceites), and ointments (pomadas) in Mexico, and a number of these products are sold freely as over-the-counter remedies for rheumatic muscle pains. It is clear that, contrary to the ample available evidence, the U.S. Congress and its advisors failed to recognize the medical value of peyote to ordinary people, and the reason for that deliberate failure was that they needed to put peyote in Schedule 1 to maximize its “scare value” to the U.S. public, so that the citizens would feel amply protected from the dangers (falsely) attributed to peyote by our beneficent legislators in their blinkered wisdom.
But such post hoc application of valid data to peyote is of little avail, as peyote is still chained in Schedule 1. And let us be clear: the fault of the classification of peyote in Schedule 1 lies squarely on the shoulders of the U.S. Congress. That scheduling of peyote was done in the same legislation that created the DEA. Once the CSA was enacted, it was incumbent upon the DEA to enforce it as best they could, despite the masses of contradictions—not merely bad science, but anti-science—that the Congress enshrined in the legislation for the political purpose of getting their anti-drug constituencies off their back.
Almost all scheduled drugs regulated under the CSA are chemical compounds that have politically unpopular pharmacological activity. There are two interesting exceptions to that generality: peyote and cannabis. In both cases, not only the principal pharmacologically active constituents of the plants, but also the whole plants (living or dead), were placed in Schedule 1 by Congress. It has recently become obvious—and becomes more obvious with virtually every valid scientific study published—that cannabis was relegated to Schedule 1 in the CSA largely because it had been relentlessly demonized in false and blatantly racist propaganda by Harry Anslinger. The winds of change are blowing favorably for cannabis now, with the plant being decriminalized for both medical and “recreational” use in about half the states of the United States. But the plant remains federally illegal in accordance with the CSA, so there is patent contradiction and friction between state law and federal law on the regulation of cannabis. However, there is talk now that Congress may act to remove cannabis from Schedule 1 of the CSA in the near future.
But where does that leave the other whole plant regulated by the CSA: peyote? While it is true that peyote, like cannabis, was politically packaged as a sheep in wolf’s clothing in the late 1960’s to ensure its classification in Schedule 1 of the CSA, reversing that original CSA classification is a more difficult task for peyote than for cannabis. The principal reasons for this include: (1) Cannabis is much better known than peyote in mainstream U.S. society and is far more widely used. Three U.S. Presidents have admitted to having smoked cannabis, and recent research indicates that 49% of the U.S. population has done likewise. In contrast, only about 2% of Americans have ever ingested peyote.13 Cannabis occurs naturally in Asia, is naturalized in the U.S., and is widely cultivated on every continent except Antarctica; whereas peyote occurs naturally only in Mexico and the U.S., and is cultivated only on a very small scale. Accordingly, peyote is less well known —and particularly less appreciated for its medicinal uses—outside of its range of natural occurrence in northeastern Mexico and adjacent Texas. (2) The potential cannabis market is huge compared to the potential market for peyote, and cannabis (a fast-growing massive annual) brings a return on investment that is far larger than what can be projected for peyote (a slow-growing small perennial requiring substantially more than a decade between seed and appropriate first harvesting). Because of (1) and (2), funding for safety and efficacy studies of new medical uses of peyote is still scarce, in contrast to the scrambling of investors to provide funding for studies of new medical uses of cannabis and its molecular constituents. (3) Although the senseless and counterproductive “War on Drugs” is now waning, there is still a great deal of ignorance and fear that is centered on the group of drugs characterized as “hallucinogens,” and peyote is still considered by some to belong to that group of psychoactive drugs. It is actually possible to find drug treatment services offered for peyote addiction,14 but it seems doubtful that such organizations have encountered any calls for their services. (N.b.: Many knowledgeable authorities argue that the term “hallucinogen” is inappropriate for peyote, and that the term “entheogen”—defined as a substance that causes the divine to become manifest within a person—is a more accurate characterization for a religious sacrament such as peyote.)
How long it will take peyote to shake off the chains of misconception associated with the War on Drugs, is unclear. However, it is not unreasonable to expect that cannabis will “clear the path” for peyote to be more widely investigated, to be more widely used, and to take its rightful place as medicine, in the pharmacopoeia as well as in the tipi.
This text was originally published at Drogas, Política y Cultura
Peyote illustration:
By Schumann, Gürke & Vaupel Peter A. Mansfeld for the filtered image. – Blühende Kakteen – Iconographia Cactacearum Tafel, 149 (cropped), Public Domain, https://commons.wikimedia.org/w/index.php?curid=1973967
Map:
The New York Public Library Digital Collections.
References
- Martin Terry, Karen L. Steelman, Tom Guilderson, Phil Dering, P., and Marvin W. Rowe, “Lower Pecos and Coahuila Peyote: New Radiocarbon Dates,” Journal of Archaeological Science 33, (2006): 1017–1021. ↩
- William Eugene Johnson, “History, Use and Effects of Peyote,” Indian School Journal 12 (1912): 239–242, 289–293. ↩
- Harry J. Anslinger and Courtney Riley Cooper, “Marijuana: Assassin of Youth,” The American Magazine 124 (July, 1937), 19–20, 150–153. ↩
- Jack Kerouac, On the Road (New York City, NY: Viking Press, 1957). ↩
- Tom Robbins, Another Roadside Attraction (New York City: Random House, 1971). ↩
- Drug Enforcement Administration, 2015. DEA Drug Info, Drug Scheduling (Washington, D. C.: US Department of Justice). www.dea.gov/druginfo/ds.shtml ↩
- US Congress. 1929. Porter Narcotic Farm Act (P.L. 70–672, 45 Stat. 1085) (See Chapter 82.) ↩
- H. Hopkins, personal communication. ↩
- John H. Halpern and Harrison G. Pope Jr., “Do Hallucinogens Cause Residual Neuropsychological Toxicity?” Drug Alcohol Depend. 53, no. 3, (1999): 247–56. ↩
- Shaun D. Carstairs and F. Lee Cantrell, “Peyote and Mescaline Exposures: A 12-Year Review of a Statewide Poison Center Database,” Clinical Toxicology 48 (2010): 350–353. ↩
- Richard Evans Schultes, 1938. The appeal of peyote (Lophophora Williamsii) as a medicine, American Anthropologist 40 (1938): 698–715; and Richard Evans Schultes, “The Aboriginal Therapeutic Uses of Lophophora Williamsii.” Cactus and Succulent Journal 12 (1940): 177–181. ↩
- See F. Hernández, Rerum medicarum Novae Hispaniae Thesaurus, Sue (Nova) Plantarum, Animalium, Mineralium Mexicanorum Historia (Rome: Mascardi, 1628 (1577); and Bernardino de Sahagun, Historia General de las Cosas de Nueva España (1829 (1582). ↩
- Teri S. Krebs and Pål-Ørjan Johansen, 2013. Over 30 Million Psychedelic Users in the United States, F1000Research 2: 98. doi: 10.12688/f1000research.2-98.v1. ↩
- Recovery.org. http://www.recovery.org/topics/choosing-the-best-inpatient-peyote-recovery-center/ ↩
Take a minute to browse our stock:
Did you enjoy reading this article?
Please support Chacruna's work by donating to us. We are an independent organization and we offer free education and advocacy for psychedelic plant medicines. We are a team of dedicated volunteers!
Can you help Chacruna advance cultural understanding around these substances?
Become a Chacruna Member
To make a direct donation click the button below:

Wednesday, June 9th, 2021 from 12-1:30pm PST
REGISTER FOR THIS EVENT HERE
There is growing enthusiasm in Jewish communities about possible ancient use and modern applications of plant medicine in Jewish spiritual development. Psychedelic Judaism introduce new potential modes of healing...





